

A familiar story plays out in clinics and group chats. Someone is gaining weight, feeling cold, dragging through afternoons, and watching their hair thin. They finally get lab work. The TSH comes back normal. The conclusion feels final. Your thyroid is fine, so your symptoms must be lifestyle, aging, or stress.
That conclusion is often too simple.
TSH is a powerful screening tool, and it is often the right first test. But it is not a direct measure of how thyroid hormone is acting inside tissues, and it is not designed to answer every question people mean when they say thyroid and metabolism. A normal TSH can coexist with issues that slow metabolic function, and an abnormal TSH can appear in situations where the thyroid gland is not the real problem.
The more useful way to read thyroid labs is to treat TSH as one signal in a larger system.
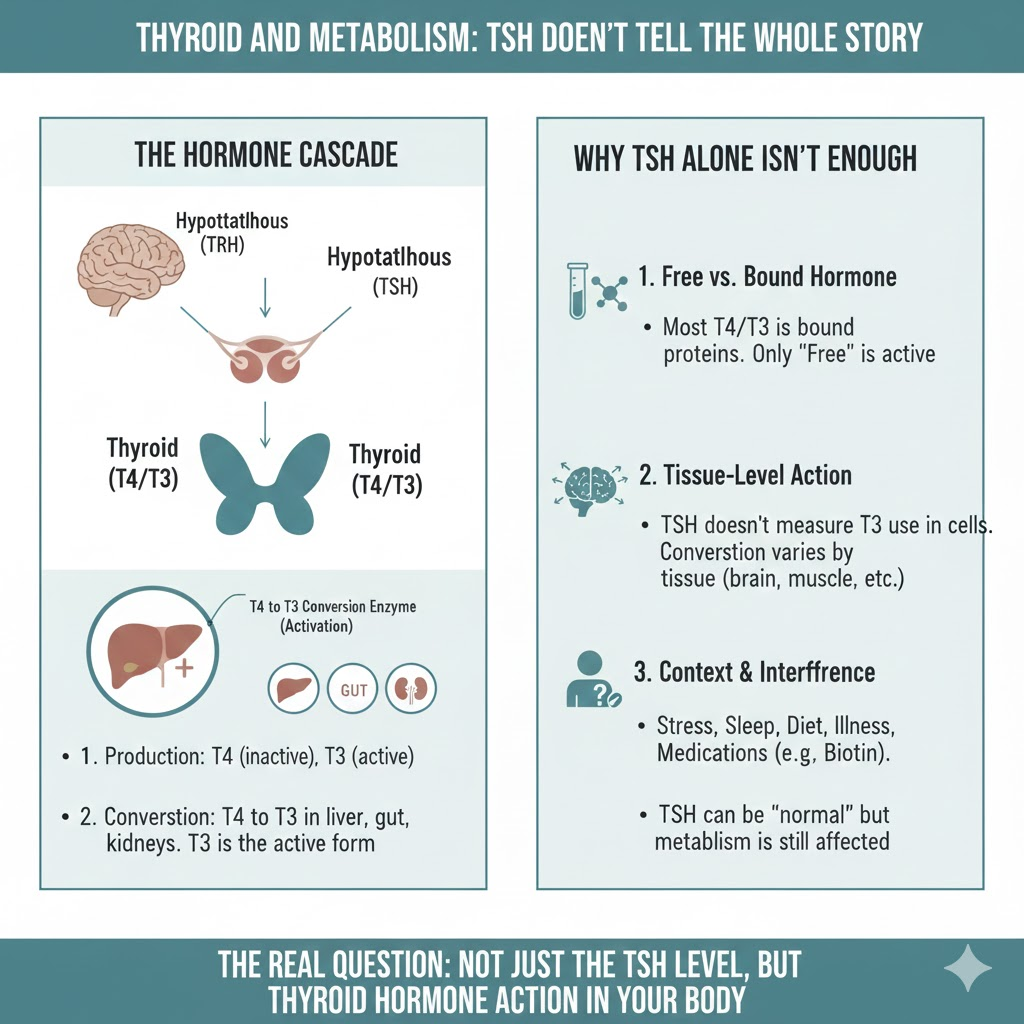
TSH is a control signal, not the end product
TSH is produced by the pituitary gland and acts like a messenger that tells the thyroid gland how hard to work. When thyroid hormone is low, TSH generally rises. When thyroid hormone is high, TSH generally falls. This feedback loop is why TSH is considered a sensitive early indicator for many forms of primary thyroid dysfunction.
But sensitivity is not the same as completeness.
TSH does not measure the amount of active thyroid hormone that reaches a specific tissue. It also does not measure how efficiently that tissue converts thyroid hormone into its active form. Those steps matter because metabolism is not controlled by one gland alone. It is controlled by hormone production, transport, conversion, and receptor signaling across many tissues.
That is the first reason TSH levels do not tell the whole story for thyroid and metabolism.
The body runs on T3 action, and most T3 is made outside the thyroid
Most people learn thyroid biology as a simple output story. The thyroid makes hormones, and those hormones set the metabolic rate. The reality is more distributed.
The thyroid produces mostly thyroxine, also called T4, and a smaller amount of triiodothyronine, also called T3. Much of the T3 the body uses is produced in other tissues through conversion from T4 by enzymes called deiodinases.
This matters because two people can have the same TSH and the same T4, yet differ in how much T3 is generated and used at the tissue level. Endotext reviews describe how T4 is metabolized through different deiodination pathways, including conversion to active T3 and to inactive metabolites, and how this metabolism is a major part of thyroid hormone turnover.
So when people say they want to understand thyroid and metabolism, they are often asking about tissue-level thyroid hormone action, not only gland-level output.
Free hormones and binding proteins can change the picture
Another reason TSH can feel disconnected from symptoms is that circulating thyroid hormone exists in different forms. Much of T4 and T3 in the blood is bound to carrier proteins, and only a small fraction is free and biologically available.
Clinical references emphasize that changes in thyroid hormone binding proteins can shift total hormone levels without changing free hormone levels, which is one reason free T4 is often used to avoid misinterpretation.
If a person looks only at one number, like TSH, they may miss a situation where free hormone, binding dynamics, or transport is part of the issue being evaluated.
When TSH can be normal but thyroid function is not
There are specific scenarios where a normal TSH does not rule out a thyroid-related problem. These are not rare edge cases in real-world practice.
Central hypothyroidism
If the pituitary or hypothalamus is not signaling normally, the thyroid gland may not be adequately stimulated even when the body needs more hormone. In central hypothyroidism, TSH can be low, normal, or sometimes not appropriately elevated, while free T4 is low. Clinical references note that normal TSH does not rule out hypothyroidism in central causes and that diagnosis relies on free T4 patterns and context.
Nonthyroidal illness and calorie deprivation
During serious illness, major surgery, or severe calorie restriction, thyroid labs can shift in ways that do not reflect primary thyroid disease. This is often called nonthyroidal illness syndrome or euthyroid sick syndrome. It can show patterns like low T3 with normal TSH and sometimes altered T4, depending on severity.
Supplement interference that makes labs look normal
High-dose biotin supplements can interfere with certain lab assays and produce misleading thyroid results on some platforms. The FDA has warned that biotin can interfere with laboratory tests and lead to incorrect results, and thyroid tests are among those that can be affected.
In each of these scenarios, the question is not whether TSH is useful. The question is whether TSH alone answers what the clinician is trying to determine about thyroid and metabolism.
Why metabolism symptoms do not map neatly to one thyroid number
People often use metabolism as shorthand for weight. That is understandable, but thyroid hormones influence more than the scale.
Authoritative endocrine sources describe thyroid hormone as central to how the body uses energy and how multiple organs function. NIDDK describes that thyroid hormones control the way the body uses energy and affect nearly every organ. The American Thyroid Association explains that thyroid hormone helps the body use energy and control metabolism and supports function across major systems.
Even in confirmed hypothyroidism, weight change is often smaller than people expect and can include water and salt retention, not only fat gain. The American Thyroid Association notes that hypothyroidism can cause some weight gain and that much of the weight gained may be due to salt and water retention.
That point changes how you interpret symptoms. If someone has stubborn weight change with a normal TSH, it does not automatically mean the thyroid is irrelevant. It means weight is an imprecise proxy for thyroid hormone action, and other metabolic drivers could be contributing.
A workplace example that shows the gap between TSH and lived metabolism
Imagine a person with a high-stress job, inconsistent sleep, and aggressive dieting. They train hard, cut calories, and rely on caffeine to push through the day. They feel colder, weaker, and more mentally foggy. Their TSH is normal.

In that scenario, the body may be adapting to stress load and energy scarcity. Thyroid hormone metabolism and signaling can shift during illness, calorie deprivation, and chronic strain, even when the thyroid gland itself is structurally normal.
A single TSH value is not built to describe that entire adaptation story. That is why many people feel dismissed when told the thyroid is fine. The better response is to interpret the thyroid tests in context and then evaluate the broader metabolic environment.
What does a more complete thyroid workup often include
When symptoms strongly suggest thyroid dysfunction or when risk is higher, clinicians commonly look beyond TSH.
Free T4 is a typical companion test because it reflects circulating thyroid hormone availability. NIDDK describes thyroid tests, including T4 tests, and how high or low T4 levels can signal thyroid conditions.
In some situations, additional testing may be relevant, such as T3 measurement when hyperthyroidism is suspected with certain patterns, and antibody testing when autoimmune thyroid disease is a concern.
This is not an argument for ordering every thyroid test for everyone. It is an argument for matching the test to the question. TSH is excellent for many questions, but not all of them.
The functional medicine debate, and the part worth keeping
A lot of online content frames thyroid care as a battle between conventional medicine and functional medicine. The most productive middle ground is simpler.
Conventional medicine is right to emphasize validated diagnoses, safety, and avoiding unnecessary treatment. At the same time, patients are right that symptoms can exist even when a screening test looks fine, and that thyroid and metabolism are a system, not a single lab value.
A useful mindset is to treat TSH as the opening chapter, not the entire book. The next chapters include free hormone availability, tissue conversion, binding, illness effects, medication and supplement interference, and the lived context of sleep, stress, and nutrition.
A lot of people first start paying attention to thyroid and metabolism through popular educators like Dr. Berg, especially when they are trying to connect fatigue, dieting, and stress with hormone patterns. The best use of that content is as a starting point for questions to discuss with a clinician, not as a replacement for proper evaluation when symptoms are significant.
The bottom line
TSH is a crucial tool, and for many people, it is the right first signal. But it is not a direct measure of thyroid hormone action in tissues, and it can be misleading in specific contexts like central hypothyroidism, serious illness, calorie deprivation, and test interference.
If you are trying to understand thyroid and metabolism, the most accurate view is at the system level. Production matters, but so does transport, conversion, and context. That is why TSH levels do not tell the whole story.